

Abstract
Background:
Myeloproliferative neoplasms (MPN) including polycythemia vera (PV), essential thrombocythemia (ET), and myelofibrosis (MF) are clonal hemopathies characterized by burdensome symptom profiles and impaired quality of life. Treatments include pharmacologic approaches, phlebotomy, and bone marrow transplant. Outcome studies have historically focused on hematologic improvement and survival benefit. Few prospective studies have evaluated patient-reported symptoms and quality of life outcomes after standard therapy. The Myeloproliferative Neoplasm Quality of Life (MPN-QOL) Study Group aims to objectively quantify symptomatic response to standard treatments. Here we provide updated results for the prospective MPN Experimental Assessment of Symptoms by Utilizing Repetitive Evaluation (MEASURE) trial.
Methods:
The MEASURE trial is a prospective international cohort study evaluating responsiveness of the Myeloproliferative Neoplasm Symptom Assessment Form Total Symptom Score (MPN-SAF TSS or MPN-10) in an anticipated 480 ET, PV, and MF patients receiving non-experimental medical therapy and/or phlebotomy.
Patients complete the MPN-SAF TSS (JCO 2012) for seven consecutive days at enrollment then again for seven days between 90 days and six months later. Patients also complete the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core-30 (EORTC QLQ-C30) and M.D. Anderson Symptom Inventory (MDASI) instruments at enrollment and on the first day of the second assessment. Physicians report demographic, laboratory, and clinical data.
Results:
Demographics
To date, 340 patients have enrolled and 270 have completed both study visits. Participants include ET (60%), PV (29%), and MF (12%; including 68% primary MF, 12% post-ET, 20% post-PV) patients. Enrolled patients are 51% male. The most common therapies received prior to enrollment were aspirin (34%), phlebotomy (15%), hydroxyurea (14%), and warfarin/clopidogrel/anticoagulation (6%). The most common current MPN therapies were hydroxyurea (67%), aspirin (24%), phlebotomy (9%), and ruxolitinib (8%). Information on mutational analysis was also collected; 77% of patients have a known JAK2 V617F mutation, 3% have an MPL W515 mutation.
Symptom Measures
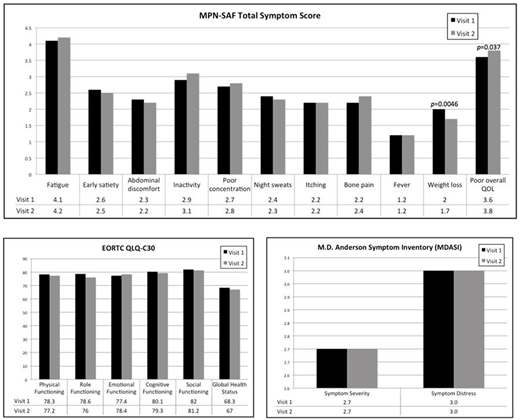
On the MPN-SAF TSS, the majority of individual symptoms assessed did not change significantly between the two assessment time points while on standard therapy. Notable exceptions were a significant decrease in weight loss (mean 2.0 vs. 1.7 on a 0=absent to 10=worst imaginable scale, p=0.005) and a significant worsening in quality of life (mean 3.6 vs. 3.8 on a 0=as good as it can be to 10=as bad as it can be scale, p=0.04). No changes were seen in other symptoms including early satiety, abdominal discomfort, night sweats, fatigue, inactivity, poor concentration, bone pain, itching, or fever. Similarly, the cumulative MPN-SAF TSS score remained stable at a mean of 24.4 over the treatment period. These findings were congruent with those observed using the EORTC QLQ-C30 instrument, with no significant changes seen in emotional, physical, role, cognitive, or social functioning. Finally, the MDASI also revealed a lack of change in either symptom severity (mean 2.7) or symptom distress (mean 3.0) scores, which remained stable over the study period.
Discussion:
Myeloproliferative neoplasms are associated with burdensome symptoms that significantly compromise quality of life. To date, no studies have quantified symptomatic response to standard-of-care treatments. Overall, results from the MEASURE study suggest that standard treatments have limited systematic impact on patient symptomatology over time, with no improvements in overall quality of life. However, we note the relatively low proportion of patients in this cohort treated with ruxolitinib, which has been shown previously to improve symptom burden, and this may have impacted the symptom responses seen in the group as whole; detailed responses by treatment and MPN subtype will be presented.
Dueck:Pfizer: Honoraria; Bayer: Employment; Phytogine: Employment. Ross:BMS: Honoraria; Novartis: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene: Research Funding. Tam:Janssen: Honoraria, Research Funding; Gilead: Honoraria; AbbVie: Honoraria, Research Funding; Pharmacyclics: Honoraria, Travel funding; AbbVie: Honoraria, Research Funding; Roche: Honoraria; Beigene: Honoraria, Other: Travel funding; Pharmacyclics: Honoraria; Gilead: Honoraria; Roche: Honoraria; Beigene: Honoraria, Other: Travel funding. Radia:Novartis: Speakers Bureau; Blueprint: Consultancy. Mesa:UT Health San Antonio - Mays Cancer Center: Employment; Celgene: Research Funding; NS Pharma: Research Funding; Pfizer: Research Funding; Gilead: Research Funding; Genentech: Research Funding; Promedior: Research Funding; CTI Biopharma: Research Funding; Incyte Corporation: Research Funding; Novartis: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal